Scarlet Fever
Definition
- An acute febrile illness caused by the pyrogenic exotoxins of Group A β-hemolytic Streptococci
Causative pathogen
- Group A β-hemolytic Streptococci
- Streptococcus pyogenes that produces pyrogenic exotoxins
Transmission route
- Direct contact with respiratory secretions of patients and carriers
- Indirect contact through hands or objects contaminated with respiratory secretions of patients and carriers
Common targets
- Occurs mainly in ages 5 to 15
Incubation period
- 1–7 days (average 2–5 days)
Clinical symptoms
- High fever (39–40 °C), sore throat, headache, vomiting, abdominal pain, etc.
- Rash: 1–2 days after fever onset, small sandpaper-like rashes appear across the body except around the mouth
- Diffuse, bright-red small papules starting on the upper trunk and spreading to the limbs, characterized by blanching when pressure is applied
- The rash usually disappears after about one week, but in about one-third of patients, skin peeling occurs after the rash subsides, which may leave scars (in areas such as the armpits, fingertips, buttocks, and nail tips).
- Face: Flushed appearance with pallor around the mouth
- Tongue: Initially covered with a grayish-white coating with prominent papillae (“white tongue”); after 2–3 days, it turns red with swollen papillae, giving the appearance of a bright “strawberry tongue.”
- Pharyngitis, mucopurulent exudate on the tonsils or posterior pharynx, cervical lymph node swelling, etc.
- Asymptomatic carrier rate: 8.5–21.9%
Complications
- Suppurative: Otitis media, cervical lymphadenitis, sinusitis, pneumonia, meningitis, etc.
- Nonsuppurative: Acute glomerulonephritis, rheumatic fever
Case fatality rate
- Less than 1%
Management
- Patient management: Isolate until 24 hours after starting antibiotic treatment.
- Contact management: In group facilities, if invasive Group A streptococcal infection, acute rheumatic fever, or post-streptococcal glomerulonephritis outbreak is suspected, consider antibiotic treatment for carriers. * Necrotizing fasciitis, toxic shock syndrome, etc.
Prevention
- No preventive vaccine available
- General prevention
- Proper hand washing
- Wash hands under running water for at least 30 seconds
- When coughing or sneezing, cover the mouth and nose with a tissue or upper sleeve
- Wear a mask if fever or respiratory symptoms are present
- Do not share personal items such as towels, cups, or utensils
Diagnosis/Reporting criteria
- Reporting scope: Patients and suspected/probable cases
- (Patient) A person who shows clinical symptoms consistent with scarlet fever and is confirmed to be infected with the infectious pathogen according to diagnostic criteria
- (Suspected case) A person suspected of having scarlet fever based on clinical symptoms and epidemiological links but without test results meeting diagnostic criteria
- (Probable case) A person suspected of having scarlet fever based on clinical symptoms and epidemiological links, with infection presumed according to diagnostic criteria for a probable case
- Diagnostic criteria
- Confirmed diagnosis
- - Isolation and identification of Streptococcus pyogenes detected in specimens (throat swab, blood)
- Presumptive diagnosis
- - Detection of specific antigens in the specimen (throat swab), including rapid diagnostic test kits
- Confirmed diagnosis
- Reporting period: Report within 24 hours
- Reporting method: Complete the notification form and report to the local public health center via web(http://eid.kdca.go.kr) entry or by fax
- Responsible department: KDCA Division of Infectious Disease Control
Annual incidence rate of scarlet fever
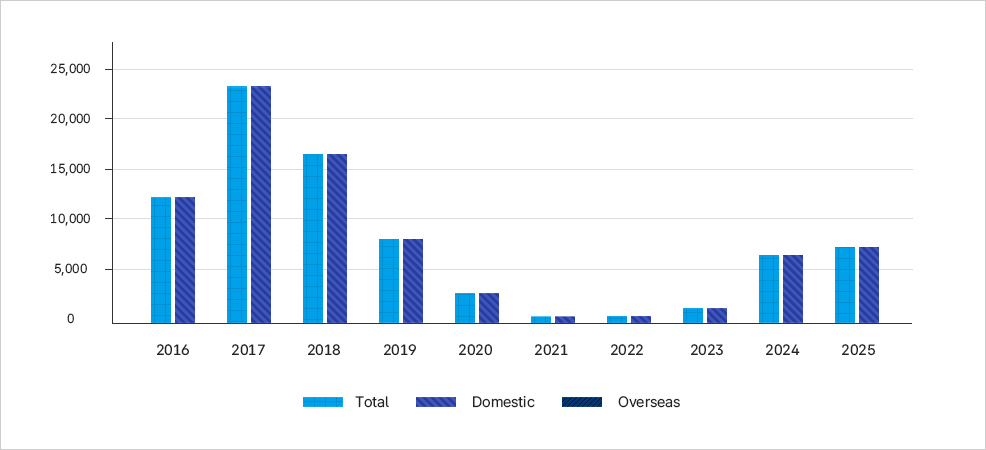
이 그래프는 2016년부터 2025년까지 성홍열 발생률을 국내와 국외로 구분하여 보여준다. - 2016년 발생 건수는 약 12,000건으로 시작하였다. - 2017년에는 약 24,000건으로 크게 증가하며 최고치를 기록하였다. - 2018년에는 약 16,000건 수준으로 감소했으나 여전히 높은 발생률을 유지하였다. - 2019년에는 약 8,000건으로 절반 수준으로 줄었고, - 2020년에는 약 3,000건 수준으로 더 감소하였다. - 2021년과 2022년은 각각 약 1,000건 내외로 최저 수준을 기록하였다. - 2023년에는 약 2,000건으로 소폭 증가하였다. - 2024년과 2025년에는 각각 약 6,000~7,000건 수준으로 다시 뚜렷한 증가세를 보였다. 전체적으로 성홍열 발생은 2017년에 정점을 찍은 뒤 코로나19 유행 시기 동안 급격히 감소했으며, 최근 다시 증가하는 추세를 나타낸다.